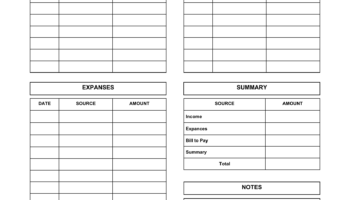
A readily available and cost-free document designed for care providers to record daily activities, observations, and vital information concerning the individual under their care. These documents typically include sections for medication administration, meals, personal hygiene, mood, activities, and any unusual events or concerns. They serve as a detailed record of the care provided. An example would be a downloadable form containing fillable fields for date, time, patient name, caregiver initials, and specific categories for documenting daily routines and health indicators.
The utilization of these resources offers several key advantages. Consistent and accurate documentation facilitates effective communication among caregivers, family members, and medical professionals. This improved communication can lead to better-informed decision-making regarding the care recipient’s health and well-being. Furthermore, it provides a historical record that can be valuable for tracking progress, identifying potential issues, and ensuring accountability in care delivery. Historically, these types of records were handwritten in notebooks, but the advent of digital technology has allowed for the creation and distribution of easily accessible templates.
The following sections will delve into the specific benefits of these resources, the types of information commonly recorded, where to find them, and how to effectively utilize them to enhance caregiving practices.